Risk penetrance estimates give a range wide enough to describe many people in many situations. You may feel overwhelmed trying to apply these general estimates to your unique situation. You don’t have to make health care choices alone. Resources are available to help.
Recommendations and guidelines
For genes known to have associated cancer risks, the National Comprehensive Cancer Network recommends prevention steps. The most extreme precautions are reserved for mutations with high risk penetrance estimates.
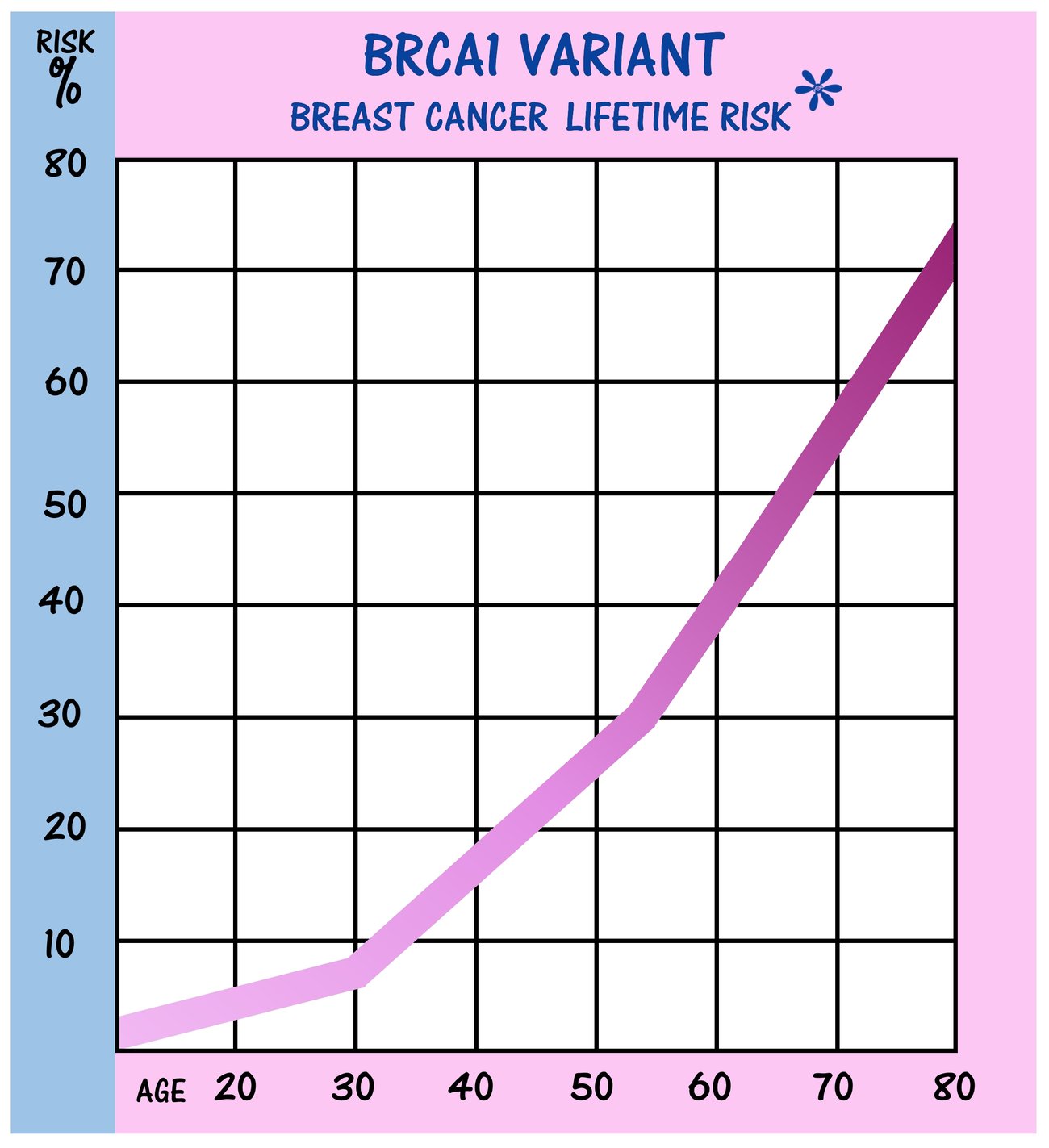
“It’s not only important for us to know that this gene has been proven over and over again that it causes cancer risk, but we also need to know that it’s high enough that the surgical prevention would be beneficial,” said certified genetic counselor Jessica Corredor. “If we see a gene that’s putting people at a 50 or higher percent risk for breast cancer, that’s when surgical prevention potentially starts being discussed.”
The American Heart Association Task Force on Clinical Practice has released guidelines that include prevention steps for hereditary hypercholesterolemia.
Genetic counselors
The guidelines for your gene might feel too extreme—or too conservative. Your gene may not have set guidelines. In these cases, a genetic counselor can talk you through a decision about treatment for cancer or heart disease.
“Is your worst-case scenario that you do have surgery that you never needed to have?” Jessica asks. “Or is your worst-case scenario that you didn’t get the surgery and you do develop a cancer, and you look back wishing you had done the surgery?”
Since genetic counselors typically spend more time with patients than doctors do, they can help those patients make decisions on their terms and at their own pace.
“If they need time to think through their decisions, to see what they feel comfortable with, in the meantime we can absolutely still screen them and give them the reassurance every few months that things are looking okay,” Jessica said.
Genetic counselors can also advise you on complicated prevention and screening situations.
“If cancer is found early,” Angela said of the brain cancer in her family, “it’s possible that the surgery to remove the tumor could cause more disability than the tumor would. Counselors can help you think about whether some screenings can improve quality of life. Is screening really helping prevent disability and morbidity or not?”
High-risk centers
Many hospitals in metropolitan areas have high-risk cancer centers that specialize in hereditary cancer treatment and prevention. A few hospitals have high-risk heart disease centers with similar services. High-risk centers are more likely to have up-to-date information than primary care providers. They can navigate the changing knowledge about genes and the unique challenges posed by individual variants. This is especially true for lesser-known genes. These centers also offer coordinated screenings, prevention and treatment. This level of coordination can help mitigate and balance the risks of treatment.
Genetics teleservices
For some patients, travel to a high-risk cancer center is not possible. Fortunately, access to medical professionals through teleservices is increasing.
“There’s some fantastic cancer genetics professionals that are available through teleservices, and I would highly recommend them as a starting place,” Angela said.
|